Tooth gaps cannot always be treated with an implant for health or other reasons. We offer you a high-quality alternative in the form of all-ceramic and partial ceramic bridges.


Tooth gaps cannot always be treated with an implant for health or other reasons. We offer you a high-quality alternative in the form of all-ceramic and partial ceramic bridges.

Just like implants, bridges are ideal for replacing missing teeth in an aesthetically pleasing and fixed manner. You can find out whether an implant or a bridge is the better solution for replacing your missing teeth with our dental gaps decision aid.
For a bridge, the neighbouring teeth of the tooth gap are reduced in a circular fashion and serve as bridge abutments for the tooth to be replaced. Once the impression has been taken, the dental technician can fabricate the bridge in the dental laboratory. We can usually complete a bridge within a week.
A bridge can either consist of a high-gold metal framework veneered with ceramic or be made of all-ceramic. Bridges made from both materials are almost indistinguishable from a natural tooth when made by an experienced technician.

3-unit CEREC bridge
3-unit, fabricated in the dental laboratory
3-unit, fabricated in the dental laboratory (CH)
The durability of a dental bridge is one of the most important questions for patients considering this type of restoration - after all, it is a significant investment in their own oral health. The good news is that a well-made and carefully maintained dental bridge can function reliably for many decades.
As a guideline, dental bridges last on average 15 to 25 years, and in many cases even longer. Several factors are decisive for the lifespan: the quality of manufacture by an experienced dental technician, the material used (all-ceramic or metal-ceramic), the quality of the abutment teeth on which the bridge rests and the patient's oral hygiene.
Today,all-ceramic bridges are considered to be particularly durable and aesthetic: the material is biocompatible, tooth-coloured and barely distinguishable from natural teeth. Metal-ceramic bridges also have an excellent long-term record and offer additional stability thanks to the metal framework - especially in the posterior region with high masticatory loads.
The greatest risk factors for a shortened lifespan are caries on the abutment teeth, gum disease (periodontitis), grinding and clenching (bruxism) and inadequate hygiene in the area of the bridge. A poorly fitting denture edge can also lead to bacteria penetrating and damaging the abutment teeth.
Regular check-ups at the dentist - at least once a year - are essential in order to assess the condition of the bridge and abutment teeth at an early stage and take countermeasures if necessary. If you also use dental floss, interdental brushes and fluoridated toothpaste every day, you will lay the foundation for a dental bridge that will last a lifetime.
Cleaning a dental bridge is more challenging than cleaning natural teeth - because there is an area under the so-called pontic (the replacement tooth that floats over the gap between the teeth) that a normal toothbrush cannot reach. If you neglect this area, you risk caries on the abutment teeth, inflammation of the gums and ultimately the loss of the bridge.
The most important cleaning instrument for a dental bridge is dental floss with a floss threader or special superfloss dental floss, which has a stiff thread at the beginning. This allows the floss to be guided under the pontic and the junction between the bridge and the gums to be thoroughly cleaned from both sides. You should carry out this step daily - it is essential.
In addition, interdental brushes in the appropriate size are recommended, which also fit under the pontic and can clean the lateral areas. A water flosser (oral irrigator) is another useful addition: it flushes bacteria and food debris out of hard-to-reach areas and can make cleaning much easier - but does not completely replace mechanical cleaning with dental floss.
Brushing around the bridge is done as usual with a toothbrush - electric or manual - and a fluoride toothpaste. Particular attention should be paid to the transition areas between the bridge and the natural tooth as well as the gum line, as plaque accumulates particularly easily there.
Professional dental cleanings by a dental hygienist every six months are particularly recommended for bridge wearers, as they can also clean areas that cannot be fully reached with home remedies. With the right care routine, your dental bridge will remain hygienic, functional and aesthetic for many years to come.
The dental bridge vs. implant comparison is one of the key decisions faced by patients with a tooth gap. Both methods have their strengths and weaknesses - the optimal choice depends on the individual situation, the health of the neighbouring teeth, the jawbone and personal preferences.
The dental bridge is the classic, tried-and-tested solution: it is anchored to the neighbouring teeth in the gap, which are ground down for this purpose. This means that healthy neighbouring teeth are permanently altered - a disadvantage that should be known in advance. On the other hand, the bridge is usually produced more quickly (often within a week) and in many cases is cheaper than an implant.
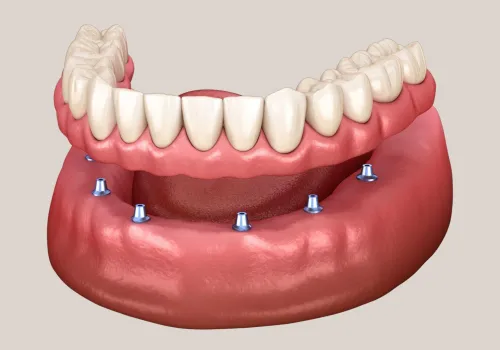
The dental implant, on the other hand, replaces the missing tooth with an artificial root replacement in the jawbone and leaves the neighbouring teeth completely untouched. It acts on the bone like a natural root and prevents the bone atrophy that typically sets in after tooth loss. This makes the implant the superior solution from a biological and long-term perspective, provided the conditions are right.
However, implants are not suitable for every patient: Too little bone, untreated general diseases, heavy smoking or certain medications can speak against an implant. In such cases, a dental bridge is the more suitable alternative.
Another aspect is time: an implant usually requires several months from implantation to the final restoration, whereas a bridge is fully inserted after just a few weeks. For patients who want an aesthetic and functional result quickly, a bridge may therefore be the more practical choice. A personalised consultation with a dentist is essential to make the right decision.
Many patients are concerned about pain when having a dental bridge fitted - understandably so, as preparing the abutment teeth involves grinding away tooth structure. The good news is that the treatment is completely painless thanks to local anaesthesia.
The most complex step in the fabrication of a dental bridge is the grinding of the abutment teeth. These are reduced circularly to create space for the bridge crowns. This procedure is carried out under local anaesthetic so that you do not feel anything during the treatment. The only things you will feel are pressure, vibration and noise - but no pain.
After the anaesthetic has worn off - usually a few hours after the treatment - the ground teeth may temporarily react sensitively, especially to cold, heat or draughts. This sensitivity is normal and in most cases subsides within a few days to weeks. If necessary, over-the-counter painkillers such as paracetamol or ibuprofen can be taken for a short time.
Between the grinding and the permanent insertion of the bridge, the abutment teeth are protected with a temporary bridge made of plastic, which covers the teeth, protects them from irritation and allows you to test your chewing comfort and aesthetics. Fitting the permanent bridge at the end is also a straightforward, painless process - the dentist checks the fit, adjusts it if necessary and then cements the bridge permanently.
If you notice persistent pain, pressure or bite problems after the permanent bridge has been fitted, do not hesitate to contact your dental practice. In many cases, a small bite correction is all that is needed to fully restore your well-being.
One aspect that is often overlooked when it comes to dental bridges and jawbones is the question of what happens to the jawbone in the gap that is bridged by the bridge in the long term. This is where the bridge differs fundamentally from the implant.
When a tooth is lost, the jawbone at this point lacks the natural stimulation from chewing forces that are normally transferred to the bone via the tooth root. As a result, the bone slowly begins to recede - a process known as bone atrophy.
With a dental bridge, the replacement tooth (the pontic) bridges the gap without penetrating the bone. The chewing forces are transferred via the abutment teeth to their roots and the neighbouring bone - but not to the bone under the gap. This means that bone loss in the gap continues even with a dental bridge, albeit at a slower rate than without any restoration.
Over the years, this bone loss can cause the gums under the pontic to recede, creating an unsightly gap between the bridge and the gums. In such cases, the bridge may need to be adjusted or remodelled years later.
The dental implant is clearly superior to the bridge in this respect, as it is anchored in the bone as an artificial root and actively prevents bone loss. If the preservation of the bone is an important criterion - for example for aesthetic reasons in the front area or in preparation for later restorations - the implant should be favoured. Your dentist will openly explain the long-term consequences of both solutions to you during your consultation.
The question of whether an old or damaged dental bridge can be renewed is one that many patients ask themselves after years of wearing it. The answer is pleasingly clear: Yes - a dental bridge can be renewed, replaced or replaced by another solution in most cases.
There are various reasons for replacing an existing dental bridge: The most common is decay on one of the abutment teeth, which has formed under the crown and is destroying the bridge's support. A fracture of the bridge - due to heavy chewing or an accident - also makes replacement necessary. Aesthetic reasons can also play a role: An old metal-ceramic bridge, where the metal edge is visible on the gums, can be replaced with a modern all-ceramic bridge.
When replacing a dental bridge, the old bridge is removed first - this is usually a straightforward procedure. The abutment teeth are then assessed: If they are intact and stable enough, they can serve as anchors again. In some cases, the preparation needs to be adjusted slightly before a new impression is taken and a new bridge is made.
If an abutment tooth is no longer suitable as a support due to caries or a fracture, the treatment strategy must be fundamentally reconsidered. Possible alternatives are then an implant in place of the lost abutment, a longer bridge with other anchor teeth or a prosthesis. In such cases, comprehensive consultation and planning with the dentist is essential.
Experience shows: If you take good care of your dental bridge and attend regular check-ups, you can expect the restoration to last a long time and avoid costly and time-consuming replacements.
The production time for a dental bridge is relatively short compared to other tooth replacement solutions - a clear advantage for patients who want a fixed restoration as quickly as possible. As a rule, two to three visits to the dentist are required for the entire bridge restoration.
At the first appointment, the abutment teeth are ground down, a precise impression of the teeth is taken and a temporary restoration is inserted to protect the ground-down teeth and bridge the aesthetic and chewing function. At the same time, the desired tooth colour and material for the permanent bridge are determined.
The impression - or a digital 3D scan in modern practices - is then sent to the dental laboratory. There, the bridge is manufactured with precision craftsmanship. This process usually takes five to ten working days, depending on the capacity utilisation of the laboratory and the complexity of the bridge.
In modern practices that have a CEREC milling machine (CAD/CAM system), a bridge can even be completed and inserted on the same day in certain cases. The bridge is milled directly in the practice on the basis of a digital scan. This option is particularly convenient and saves an additional visit to the practice.
At the second appointment, the finished bridge is tried in, checked for fit and bite and adjusted if necessary. If everything fits perfectly, it is permanently fixed with a special cement. The entire process from initial grinding to final insertion usually takes one to two weeks with classic laboratory production - a remarkably short time for a fixed, long-lasting dental restoration.
When most people hear the term dental bridge, they think of the classic three-unit bridge - but there are actually different types of dental bridges that are used for different clinical situations. This overview helps to better understand the dentist's recommendation.
The conventional bridge is the most common form: it consists of two bridge crowns (on the abutment teeth) and one or more bridge units (the replacement teeth) that bridge the gap between the teeth. This variant is used when there are healthy teeth on both sides of the gap that can serve as abutments.
The free-end bridge (extension bridge) is used when an abutment tooth is only present on one side of the gap. It is technically more demanding and requires careful indication, as the one-sided transmission of force places greater stress on the abutment tooth.
The adhesive bridge (Maryland bridge) is a particularly tooth-friendly variant: the bridge pontic is not anchored by completely crowned abutment teeth, but by metallic or ceramic wings that are bonded to the inner surfaces of the neighbouring teeth. This method is particularly suitable for anterior teeth if the abutment teeth are healthy and intact and as little substance as possible is to be removed.
The implant-supported bridge is a combination of implantology and the bridge technique: Several missing teeth are replaced by implants to which a bridge is attached - without having to use natural teeth as abutments. This method offers maximum stability and bone protection. Your dentist will determine which type of bridge is suitable for you after a comprehensive examination and planning.
The question of whether health insurance in Switzerland will cover the cost of a dental bridge is one that concerns many patients - especially as the cost of a dental bridge can be considerable. Unfortunately, the answer is sobering for most patients.
Compulsory health insurance (KVG, basic insurance) does not generally cover dental treatment in Switzerland - and this also applies to dental bridges. Exceptions only exist in very specific situations: if the tooth loss is due to a serious general illness (such as certain cancers, epilepsy or severe developmental disorders), or if the illness is a necessary side effect of medically indicated treatment. These exceptions are clearly defined and only affect a small proportion of patients.
In the event of an accident - whether a leisure accident or an occupational accident - the accident insurance (UVG) in Switzerland typically covers the costs of the necessary dental treatment, provided that the accident has been reported accordingly. It is worth contacting the insurance company as soon as possible.
Supplementary dental insurance can cover part of the bridge costs, depending on the policy. Some supplementary insurance policies cover dental treatment up to a certain maximum annual amount. It is strongly recommended that you enquire with your health insurance company before starting treatment as to whether a cost contribution is possible and obtain a written cost approval.
As the costs of bridges in Switzerland usually have to be borne privately, many practices - including CITYDENTAL - offer transparent quotes and instalment payment options where possible. A personal consultation clarifies all cost issues in advance and gives you the necessary certainty for your decision.
A dental bridge is a proven and reliable solution for missing teeth - but like any medical treatment, it also has disadvantages and risks that patients should be aware of before making an informed decision.
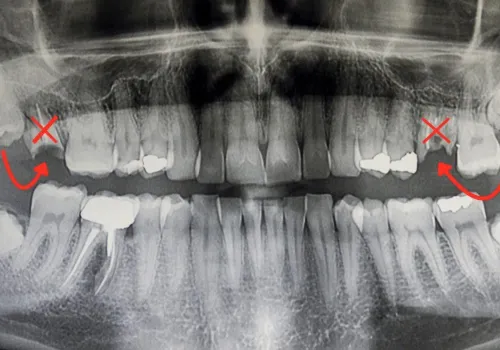
The most serious disadvantage of a conventional dental bridge is the need to grind down the abutment teeth. In order to be able to attach the bridge crowns, the neighbouring teeth must be circularly and irrevocably ground down - even if they are completely healthy and caries-free. This means that healthy tooth substance is permanently sacrificed. This procedure cannot be reversed and increases the long-term risk of the abutment teeth becoming more sensitive, caries developing under the crown or the teeth also causing problems in later years.
Another risk is the development of caries under the bridge crowns: If microscopic leaks develop between the crown margin and the tooth, bacteria can penetrate and spread unnoticed - until massive caries develops on the abutment tooth. Regular X-ray checks are therefore essential in order to recognise such developments at an early stage.
As already explained, the dental bridge does not protect the jawbone under the gap from receding. In the long term, this can lead to a change in the gum profile and to aesthetic losses.
In patients with bruxism (teeth grinding or clenching), the bridge is exposed to increased stress, which increases the risk of fracture. A grinding or occlusal splint can reduce the risk.
Finally, cleaning under the pontic is more complex than with natural teeth, which increases the risk of gum problems if care is neglected. If you are aware of the advantages and disadvantages and are prepared to invest in the necessary care, you can still be satisfied with a dental bridge for decades.